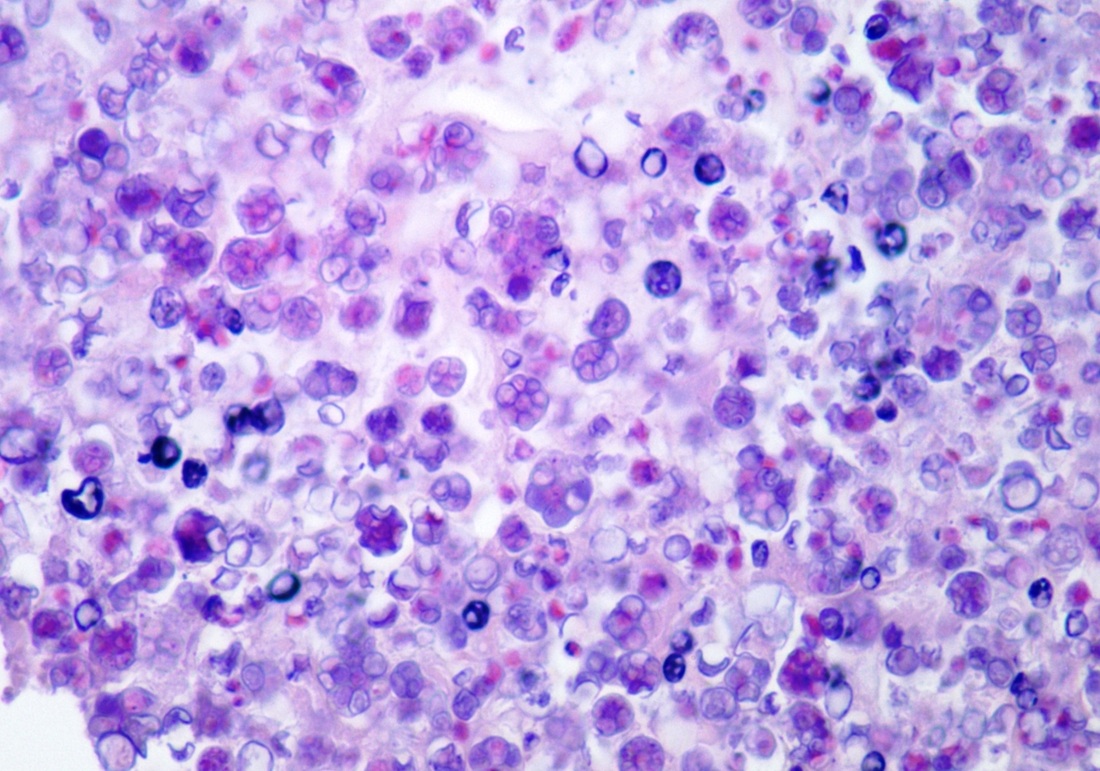
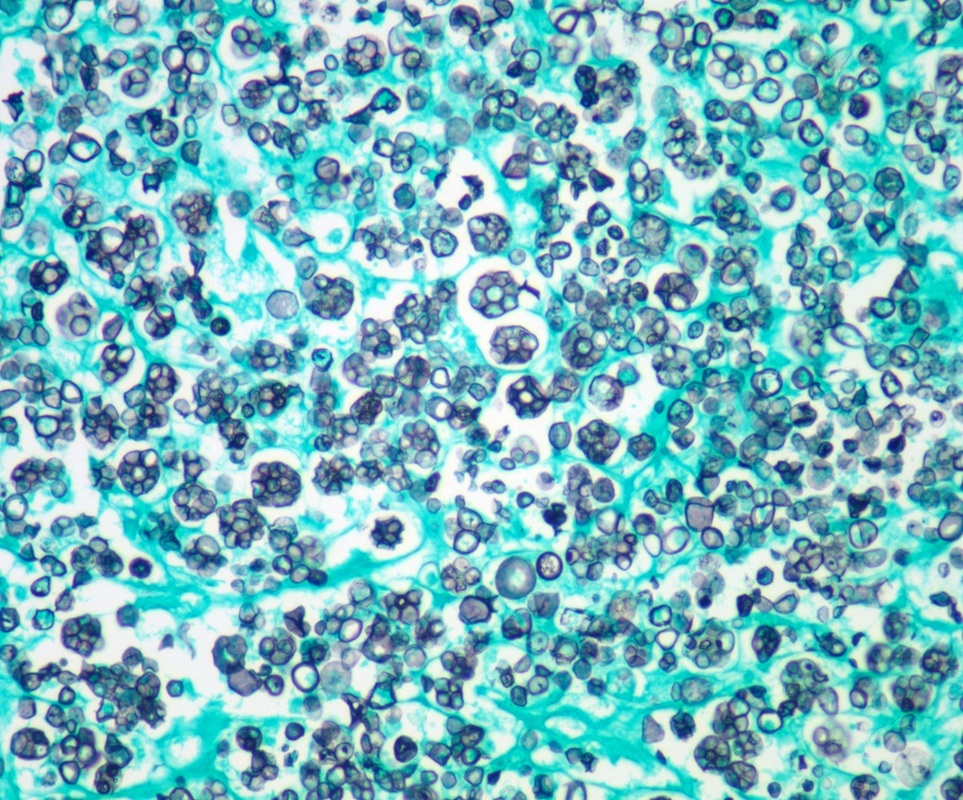
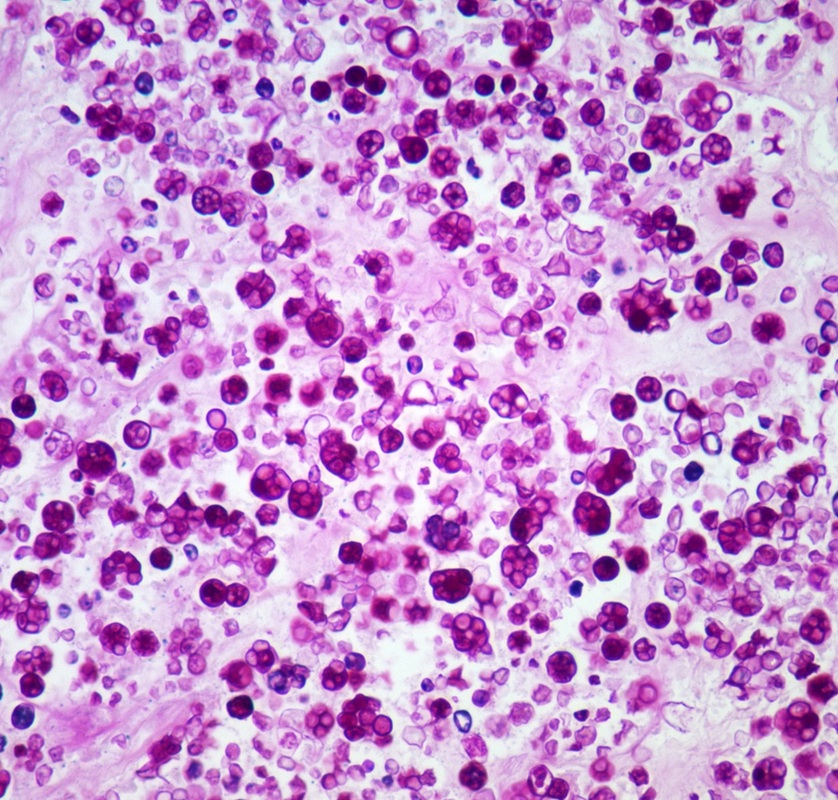
Protothecosis
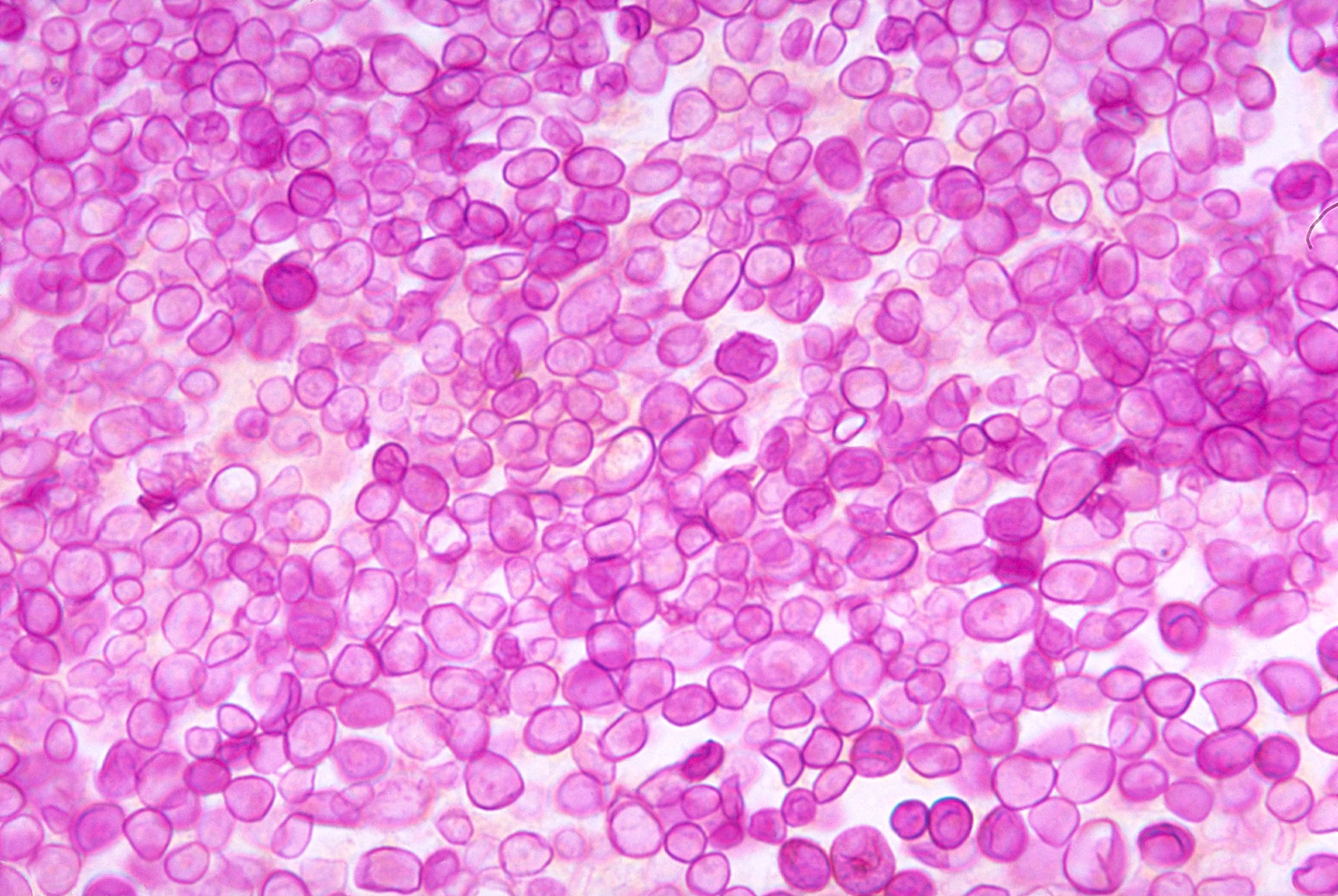
Histologic stain of a Prototheca zopfii infection in a dog
Protothecosis is a disease found in dogs, cats, cattle, and humans caused by a type of green alga known as Prototheca that lacks chlorophyll. It and its close relative Helicosporidium are unusual in that they are actually green algae that have become parasites. The two most common species are Prototheca wickerhamii and Prototheca zopfii. Both are known to cause disease in dogs, while most human cases are caused by P. wickerhami. Prototheca is found worldwide in sewage and soil. Infection is rare despite high exposure, and can be related to a defective immune system. In dogs, females and Collies are most commonly affected.
The first human case was identified in 1964 in Sierra Leone.
The first human case was identified in 1964 in Sierra Leone.
Treatment
Treatment with amphotericin B has been reported.
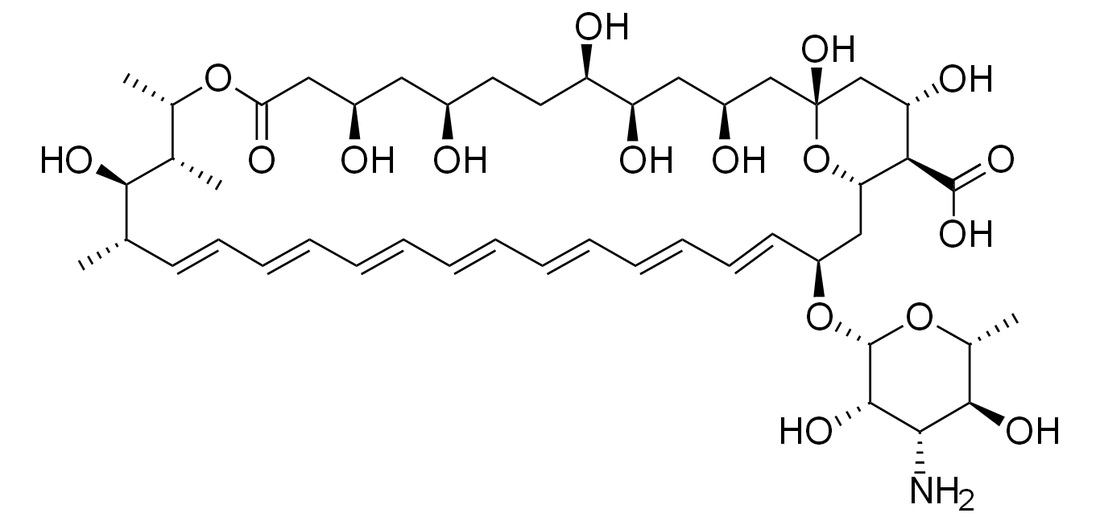
Amphotericin B (Fungilin, Fungizone, Abelcet, AmBisome, Fungisome, Amphocil, Amphotec) is a polyene antifungal drug, often used intravenously for systemic fungal infections. It was originally extracted from Streptomyces nodosus, a filamentous bacterium, in 1955 at the Squibb Institute for Medical Research from cultures of an undescribed streptomycete isolated from the soil collected in the Orinoco River region of Venezuela. Its name originates from the chemical's amphoteric properties. Two amphotericins, amphotericin A and amphotericin B are known, but only B is used clinically, because it is significantly more active in vivo. Amphotericin A is almost identical to amphotericin B (having a double C=C bond between the 27th and 28th carbons), but has little antifungal activity. Currently, the drug is available as plain amphotericin B, as a cholesteryl sulfate complex (ABCD), as a lipid complex (ABLC), and as a liposomal formulation (LAmB). The latter formulations have been developed to improve tolerability for the patient, but may show considerably different pharmacokinetic characteristics compared to plain amphotericin B.
Biosynthesis
The natural route to synthesis includes polyketide synthase components.
Uses
Antifungal
Oral preparations of amphotericin B are used to treat thrush; these are virtually nontoxic, in contrast to typical intravenous therapy (IV) doses.
One of the main intravenous uses is in treating various systemic fungal infections (e.g., in critically ill, comorbidly infected or immunocompromised patients), including cryptococcal meningitis.
Amphotericin B is also commonly used in tissue culture to prevent fungi from contaminating cell cultures. It is usually sold in a concentrated solution, either on its own or in combination with the antibiotics penicillin and streptomycin.
Antiprotozoan
Another IV use is as a drug of last resort in otherwise-untreatable parasitic protozoan infections such as visceral leishmaniasis and primary amoebic meningoencephalitis.
Mechanism of action
As with other polyene antifungals, amphotericin B binds with ergosterol, a component of fungal cell membranes, forming a transmembrane channel that leads to monovalent ion (K+, Na+, H+ and Cl−) leakage, which is the primary effect leading to fungal cell death. Recently, however, researchers found evidence that pore formation is not necessarily linked to cell death The actual mechanism of action may be more complex and multifaceted.
Mechanism of toxicity
Mammalian and fungal membranes both contain sterols, a primary membrane target for amphotericin B. Because mammalian and fungal membranes are similar in structure and composition, this is one mechanism by which amphotericin B causes cellular toxicity. Amphotericin B molecules can form pores in the host membrane as well as the fungal membrane. This impairment in membrane barrier function can have lethal effects. Bacteria are not affected as their cell membrane does not contain sterols.
Amphotericin administration is limited by infusion-related toxicity. This is thought to result from innate immune production of proinflammatory cytokines.
Side-effects
Amphotericin B is well known for its severe and potentially lethal side-effects. Very often, a serious acute reaction after the infusion (1 to 3 hours later) is noted, consisting of high fever, shaking chills, hypotension, anorexia, nausea, vomiting, headache, dyspnea and tachypnea, drowsiness, and generalized weakness. This reaction sometimes subsides with later applications of the drug, and may in part be due to histamine liberation. An increase in prostaglandin synthesis may also play a role. This nearly universal febrile response necessitates a critical (and diagnostically difficult) professional determination as to whether the onset of high fever is a novel symptom of a fast-progressing disease, or merely the induced effect of the drug. To decrease the likelihood and severity of the symptoms, initial doses should be low, and increased slowly. Acetaminophen, pethidine, diphenhydramine, and/or hydrocortisone have all been used to treat or prevent the syndrome, but the prophylactic use of these drugs is often limited by the patient's condition.
Intravenously administered amphotericin B has also been associated with multiple organ damage in therapeutic doses. Nephrotoxicity (kidney damage) is a frequently reported side-effect, and can be severe and/or irreversible. It is much milder when delivered via liposomes (AmBisome), and this is, therefore, the preferred method (see below). The integrity of the liposome is disrupted when it binds to the fungal cell wall, but is not affected by the mammalian cell membrane, thus less toxicity is seen. The association with liposomes decreases the exposure of the kidneys to amphotericin B, which explains less nephrotoxic effects. In addition, electrolyte imbalances (e.g., hypokalemia and hypomagnesemia) may also result. In the liver, increased liver enzymes and hepatotoxicity (up to and including fulminant liver failure) are common. In the circulatory system, several forms of anemia and other blood dyscrasias (leukopenia, thrombopenia), serious cardiac arrhythmias (including ventricular fibrillation), and even frank cardiac failure have been reported. Skin reactions, including serious forms, are also possible.
Interactions
Clinical efficacy
Liposomal amphotericin B was effective as empirical therapy or as treatment for confirmed invasive fungal infections in several randomized, double-blind trials (n = 73 − 1095) in adult and pediatric patients.
Liposomal and lipid complex preparations
From studies, it appears that liposomal amphotericin B preparations exhibit fewer side-effects, while having similar efficacy. Various preparations have recently been introduced. All of these are more expensive than plain amphotericin B.
AmBisome is a liposomal formulation of amphotericin B for injection, developed by NeXstar Pharmaceuticals (acquired by Gilead Sciences in 1999). It is marketed by Gilead in Europe and licensed to Astellas Pharma (formerly Fujisawa Pharmaceuticals) for marketing in the USA, and Sumitomo Pharmaceuticals in Japan.
Fungisome is a liposomal complex of amphotericin B, and being the latest and cheapest addition to the lipid formulations of amphotericin B, it has many advantages. It is marketed by Lifecare Innovations of India. Other formulations include Amphotec (Intermune) and Abelcet (Sigma-Tau Pharmaceuticals). Abelcet is not a liposomal preparation but rather a lipid complex preparation. Ampholip is a lipid complex formulation of amphotericin B marketed by Bharat Serums & Vaccines Ltd, Mumbai, India.
Oral preparations
A major barrier to the use of amphotericin in resource-poor settings is that it must be given intravenously (except for topical applications). An oral preparation exists, but is not yet commercially available.
Biosynthesis
The natural route to synthesis includes polyketide synthase components.
Uses
Antifungal
Oral preparations of amphotericin B are used to treat thrush; these are virtually nontoxic, in contrast to typical intravenous therapy (IV) doses.
One of the main intravenous uses is in treating various systemic fungal infections (e.g., in critically ill, comorbidly infected or immunocompromised patients), including cryptococcal meningitis.
Amphotericin B is also commonly used in tissue culture to prevent fungi from contaminating cell cultures. It is usually sold in a concentrated solution, either on its own or in combination with the antibiotics penicillin and streptomycin.
Antiprotozoan
Another IV use is as a drug of last resort in otherwise-untreatable parasitic protozoan infections such as visceral leishmaniasis and primary amoebic meningoencephalitis.
Mechanism of action
As with other polyene antifungals, amphotericin B binds with ergosterol, a component of fungal cell membranes, forming a transmembrane channel that leads to monovalent ion (K+, Na+, H+ and Cl−) leakage, which is the primary effect leading to fungal cell death. Recently, however, researchers found evidence that pore formation is not necessarily linked to cell death The actual mechanism of action may be more complex and multifaceted.
Mechanism of toxicity
Mammalian and fungal membranes both contain sterols, a primary membrane target for amphotericin B. Because mammalian and fungal membranes are similar in structure and composition, this is one mechanism by which amphotericin B causes cellular toxicity. Amphotericin B molecules can form pores in the host membrane as well as the fungal membrane. This impairment in membrane barrier function can have lethal effects. Bacteria are not affected as their cell membrane does not contain sterols.
Amphotericin administration is limited by infusion-related toxicity. This is thought to result from innate immune production of proinflammatory cytokines.
Side-effects
Amphotericin B is well known for its severe and potentially lethal side-effects. Very often, a serious acute reaction after the infusion (1 to 3 hours later) is noted, consisting of high fever, shaking chills, hypotension, anorexia, nausea, vomiting, headache, dyspnea and tachypnea, drowsiness, and generalized weakness. This reaction sometimes subsides with later applications of the drug, and may in part be due to histamine liberation. An increase in prostaglandin synthesis may also play a role. This nearly universal febrile response necessitates a critical (and diagnostically difficult) professional determination as to whether the onset of high fever is a novel symptom of a fast-progressing disease, or merely the induced effect of the drug. To decrease the likelihood and severity of the symptoms, initial doses should be low, and increased slowly. Acetaminophen, pethidine, diphenhydramine, and/or hydrocortisone have all been used to treat or prevent the syndrome, but the prophylactic use of these drugs is often limited by the patient's condition.
Intravenously administered amphotericin B has also been associated with multiple organ damage in therapeutic doses. Nephrotoxicity (kidney damage) is a frequently reported side-effect, and can be severe and/or irreversible. It is much milder when delivered via liposomes (AmBisome), and this is, therefore, the preferred method (see below). The integrity of the liposome is disrupted when it binds to the fungal cell wall, but is not affected by the mammalian cell membrane, thus less toxicity is seen. The association with liposomes decreases the exposure of the kidneys to amphotericin B, which explains less nephrotoxic effects. In addition, electrolyte imbalances (e.g., hypokalemia and hypomagnesemia) may also result. In the liver, increased liver enzymes and hepatotoxicity (up to and including fulminant liver failure) are common. In the circulatory system, several forms of anemia and other blood dyscrasias (leukopenia, thrombopenia), serious cardiac arrhythmias (including ventricular fibrillation), and even frank cardiac failure have been reported. Skin reactions, including serious forms, are also possible.
Interactions
- Flucytosine: Toxicity of flucytosine is increased and allows a lower dose of amphotericin B. Amphotericin B may also facilitate entry of flucystosine into the fungal cell by interfering with the permeability of the fungal cell membrane.
- Diuretics or cisplatin: Increased renal toxicity and increased risk of hypokalemia
- Corticosteroids: Increased risk of hypokalemia
- Cytostatic drugs: Increased risk of kidney damage, hypotension and bronchospasms
- Other nephrotoxic drugs (like Aminoglycosides) : Increased risk of serious renal damage, monitor kidney function closely
- Foscarnet, ganciclovir, tenofovir, adefovir: Risk of hematological and renal side-effects of amphotericin B are increased.
- Transfusion of leukocytes : Risk of pulmonal (lung) damage occurs. Space the intervals between the application of amphotericin B and the transfusion, and monitor pulmonary function.
Clinical efficacy
Liposomal amphotericin B was effective as empirical therapy or as treatment for confirmed invasive fungal infections in several randomized, double-blind trials (n = 73 − 1095) in adult and pediatric patients.
Liposomal and lipid complex preparations
From studies, it appears that liposomal amphotericin B preparations exhibit fewer side-effects, while having similar efficacy. Various preparations have recently been introduced. All of these are more expensive than plain amphotericin B.
AmBisome is a liposomal formulation of amphotericin B for injection, developed by NeXstar Pharmaceuticals (acquired by Gilead Sciences in 1999). It is marketed by Gilead in Europe and licensed to Astellas Pharma (formerly Fujisawa Pharmaceuticals) for marketing in the USA, and Sumitomo Pharmaceuticals in Japan.
Fungisome is a liposomal complex of amphotericin B, and being the latest and cheapest addition to the lipid formulations of amphotericin B, it has many advantages. It is marketed by Lifecare Innovations of India. Other formulations include Amphotec (Intermune) and Abelcet (Sigma-Tau Pharmaceuticals). Abelcet is not a liposomal preparation but rather a lipid complex preparation. Ampholip is a lipid complex formulation of amphotericin B marketed by Bharat Serums & Vaccines Ltd, Mumbai, India.
Oral preparations
A major barrier to the use of amphotericin in resource-poor settings is that it must be given intravenously (except for topical applications). An oral preparation exists, but is not yet commercially available.
The organism
Prototheca has been thought to be a mutant of Chlorella, a type of single-celled green alga. However, while Chlorella contains galactose and galactosamine in the cell wall, Prototheca lacks these. Also, Chlorella obtains its energy through photosynthesis, while Prototheca is saprotrophic, feeding on dead and decaying organic matter. When Prototheca was first isolated from slime flux of trees in 1894, it was thought to be a type of fungus. Its size varies from 2 to 15 micrometres.
Protothecosis in cattle
Cattle can be affected by protothecal enteritis and mastitis. Protothecal mastitis is endemic worldwide, although most cases of infected herds have been reported in Germany, the United States, and Brazil.
Protothecosis in dogs
Disseminated protothecosis is most commonly seen in dogs. The algae enters the body through the mouth or nose and causes infection in the intestines. From there it can spread to the eye, brain, and kidneys. Symptoms can include diarrhea, weight loss, weakness, inflammation of the eye (uveitis), retinal detachment, ataxia, and seizures.
Dogs with acute blindness and diarrhea that develop exudative retinal detachment should be assessed for protothecosis. Diagnosis is through culture or finding the organism in a biopsy, cerebrospinal fluid, vitreous humour, or urine. Treatment of the disseminated form in dogs is very difficult, although use of antifungal medication has been successful in a few cases. Prognosis for cutaneous protothecosis is guarded and depends on the surgical options. Prognosis for the disseminated form is grave. This may be due to delayed recognition and treatment.
Dogs with acute blindness and diarrhea that develop exudative retinal detachment should be assessed for protothecosis. Diagnosis is through culture or finding the organism in a biopsy, cerebrospinal fluid, vitreous humour, or urine. Treatment of the disseminated form in dogs is very difficult, although use of antifungal medication has been successful in a few cases. Prognosis for cutaneous protothecosis is guarded and depends on the surgical options. Prognosis for the disseminated form is grave. This may be due to delayed recognition and treatment.
